Guidelines on Prescribing Specialist Infant Formulas in primary care
|
|
|
- Amie Lambert
- 6 years ago
- Views:
Transcription
1 Oxfordshire Clinical Commissioning Group Guidelines on Prescribing Specialist Infant Formulas in primary care Contents 1. Introduction 2. Prescribing Guidance 2.1 Quantities to Prescribe 2.2 Prescription Management 3. Cow s Milk Protein Allergy (CMPA) 3.1 Background Information 3.2 Diagnosis and Initial Management of CMPA IgE mediated CMPA Non-IgE mediated CMPA and Home Reintroduction 3.3 Ongoing Management of Confirmed Mild to Moderate CMPA 3.4 Product choices Extensively Hydrolysed Formula (EHf) Amino Acid Formula (AAf) Products Not Suitable for Prescribing in CMPA 3.5 Prescription Management 3.6 Reintroducing Cow s Milk 3.7 Weaning 4. Gastro-oesophageal Reflux Disease (GORD) 5. Secondary Lactose Intolerance 6. Faltering Growth 7. Preterm Infants 8. Metabolic Products 9. References and Acknowledgements 10. Appendices 10.1 Appendix 1 Suspected Cow s Milk Allergy (CMA) in the 1 st Year of Life (imap) 10.2 Appendix 2 Primary Care Management of Mild to Moderate Non-IgE CMA (imap) 10.3 Appendix 3 Parent leaflet: The imap Milk Allergy Guideline Initial Fact Sheet 10.4 Appendix 4 Parent leaflet: The Early Home Reintroduction to confirm the diagnosis of cow s milk allergy 10.5 Appendix 5 The imap Milk Ladder 10.6 Appendix 6 - Infant Formula products quick reference guide 10.7 Appendix 7 Summary of Guidelines on prescribing specialist infant formula in primary care
2 1. Introduction These guidelines outline recommendations for the safe, appropriate and cost-effective prescribing of specialist infant formula for children up to the age of 18 months in the Oxfordshire area. It covers: Over-the-counter (OTC) products available wherever appropriate Quantities to prescribe Which products to use for different clinical conditions Initiating, reviewing and discontinuing prescriptions When to refer to dietitians and/ or secondary or specialist care For allergy related queries please contact consultant-led paediatric allergy advice service via Breast milk remains the optimal nutrition for infants and should be promoted, supported and encouraged where it is clinically safe. 2. Prescribing Guidance 2.1 Quantity of Powdered Formula to Prescribe When prescribing powdered infant formulas please refer to the table below for suggested quantity to prescribe per month: Age of child Suggested quantity of powdered formula to prescribe per month 400g tin 900g tin < 6 months Up to 12 tins Up to 5 tins Highest requirement at 4-6 months prior to weaning 6 12 months 6 12 tins 3 5 tins > 12 months Up to 6 tins Up to 3 tins 2.2 Prescription Management 1. Only prescribe 1-2 tins initially as acute prescription to assess tolerance and to avoid waste. Review recent correspondence from the paediatrician or paediatric dietitian. 2. Add formula to repeat prescribing template only if tolerance and diagnosis are confirmed, and a regular, robust review process is established to ensure that the formula and quantity prescribed are appropriate for the child s age and nutritional requirements. 3. Prescribing specialist formula for children over 18 months will be low priority unless specifically requested from a specialist (paediatrician or dietitian) and reason for continued use is provided, in line with Clinical Commissioning Policy DO NOT prescribe the following on NHS prescriptions. Parents should be advised to purchase these as their costs are similar to that of cow s milk formula, in line with Clinical Commissioning Policy 88 and 250: Soya formula - Wysoy 2
3 Lactose free formula - Aptamil LF, SMA LF, Enfamil O-Lac Pre-thickened formula - Cow and Gate Anti-reflux, Aptamil Anti-reflux, SMA PRO Antireflux Thickening formula - SMA Staydown (replaced by SMA PRO Anti-reflux), Enfamil AR 5. DO NOT prescribe ready-to-feed liquids as they have no clinical advantage and are usually substantially more expensive. These should only be prescribed on specialist s request when there is a clinical need e.g. if the patient is tube or PEG (percutaneous endoscopic gastrostomy) fed. 6. Prescriptions must be endorsed ACBS. 3. Cow s Milk Protein Allergy (CMPA) 3.1 Background Information CMPA is the commonest food allergy in the first year of life with a prevalence of 2-3 %. Most infants with CMPA develop symptoms within one week of introduction of a cow s milk protein (CMP) - based formula and improve within 1-2 weeks of a CMP elimination diet. However, this can take up to 6 weeks. Most children with a diagnosis of CMPA have mild to moderate symptoms which can be managed in primary care. Severe CMPA should be managed in conjunction with a paediatrician with an interest in allergy. For detailed assessment of severity of CMPA refer to imap CMPA algorithm for symptoms presentation (see appendix 1) and algorithm for diagnosis and management (see appendix 2). 3.2 Diagnosis and Initial Management of CMPA There are two main types of cow s milk allergy: acute Immunoglobulin E (IgE) mediated reactions (symptom onset within minutes up to 2 hours) and the delayed non-ige mediated reactions (2-72hrs onset). The table below depicts recognised clinical features of CMPA. For detailed guidance on obtaining an allergy focused history, see NICE CG116: Food Allergy in Children and imap allergy focused clinical history for suspected CMPA in infancy. Download the imap Milk Allergy Guideline Initial Fact Sheet (see Appendix 3) for parents whose infants are showing mild to moderate symptoms of delayed non Ig-E mediated reaction to CMP. The skin The gastrointestinal system Acute IgE-mediated Pruritus Erythema Acute urticaria localised or generalised Acute angioedema of lips, face and around the eyes Oral pruritus Colicky abdominal pain Vomiting Diarrhoea Delayed non-ige-mediated Pruritus Erythema Atopic dermatitis Gastro-oesophageal reflux Loose or frequent stools Blood and/or mucus in stools Abdominal pain Infantile colic Food refusal or aversion Constipation Perianal redness 3
4 The respiratory system (usually in combination with one or more of skin and GI symptoms) Upper respiratory tract symptoms (nasal itching, sneezing, rhinorrhoea or congestion (with or without conjunctivitis), signs or symptoms of anaphylaxis e.g. laryngeal oedema with drooling and hoarse voice and tongue swelling. Lower respiratory tract symptoms (cough, chest tightness, wheezing or shortness of breath) Note: this list is not exhaustive. The absence of these symptoms does not exclude food allergy IgE mediated CMPA (symptom onset within minutes up to 2 hours) Acute Onset symptoms: IgE mediated Mild to moderate More than one of the following symptoms: acute pruritus, erythema, urticaria, angioedema, acute flaring of atopic dermatitis, vomiting, diarrhoea, acute rhinitis Severe Immediate reactions with severe respiratory +/- CVS (cardiovascular system) signs and symptoms. Anaphylaxis -> A&E. Allergy referral and commence on AAf and dairy free weaning with dietetic support. Exclusively formula feeding: Trial EHf; Mixed feeding**: EHf top-ups if needed + maternal dairy free diet* if persistent GI symptoms or active atopic dermatitis with breast feeding** (see notes below). Any immediate symptoms on EHf feeds? Yes No Refer to specialist for allergy Continue EHf. testing to confirm CMPA and Refer for allergy plan for reintroduction, AAf testing and may be needed. Do not Reintroduction perform Home plan. Refer to Reintroduction. Refer to dietitian for dietitians for weaning support. weaning support. Exclusively breastfed: Maternal dairy free diet* for 2-4 weeks. Recurrence of immediate symptoms despite maternal dairy free diet*? Yes Refer for allergy testing to confirm CMPA. Do not Perform Home Reintroduction. Refer to dietitians for weaning support. No Mixed/ formula feeding: Urgent referral to paediatric allergy service. Formula feeding: Specialist to recommend/ commence AAf exclusively; Mixed feeding: AAf as top-ups if required. Maternal dairy free diet* if persistent GI symptoms and atopic dermatitis. Specialist follow up and Reintroduction plan. Continue maternal dairy free diet*. Refer for allergy testing and Reintroduction plan. If top-up formula required refer to paediatric allergy service for AAf. Refer to dietitians for weaning support. * Breastfeeding mothers on a milk free diet may require supplementation with 1000mg calcium and 10mcg Vitamin D per day. **Note: if no delayed symptoms prior to a mild/moderate acute reaction there is no need for maternal dairy exclusion. Rarely there may be minor immediate symptoms such as redness, hives after breast feeds. Maternal dairy free diet will be required in these cases. AAf = amino acid formula; EHf = extensively hydrolysed formula 4
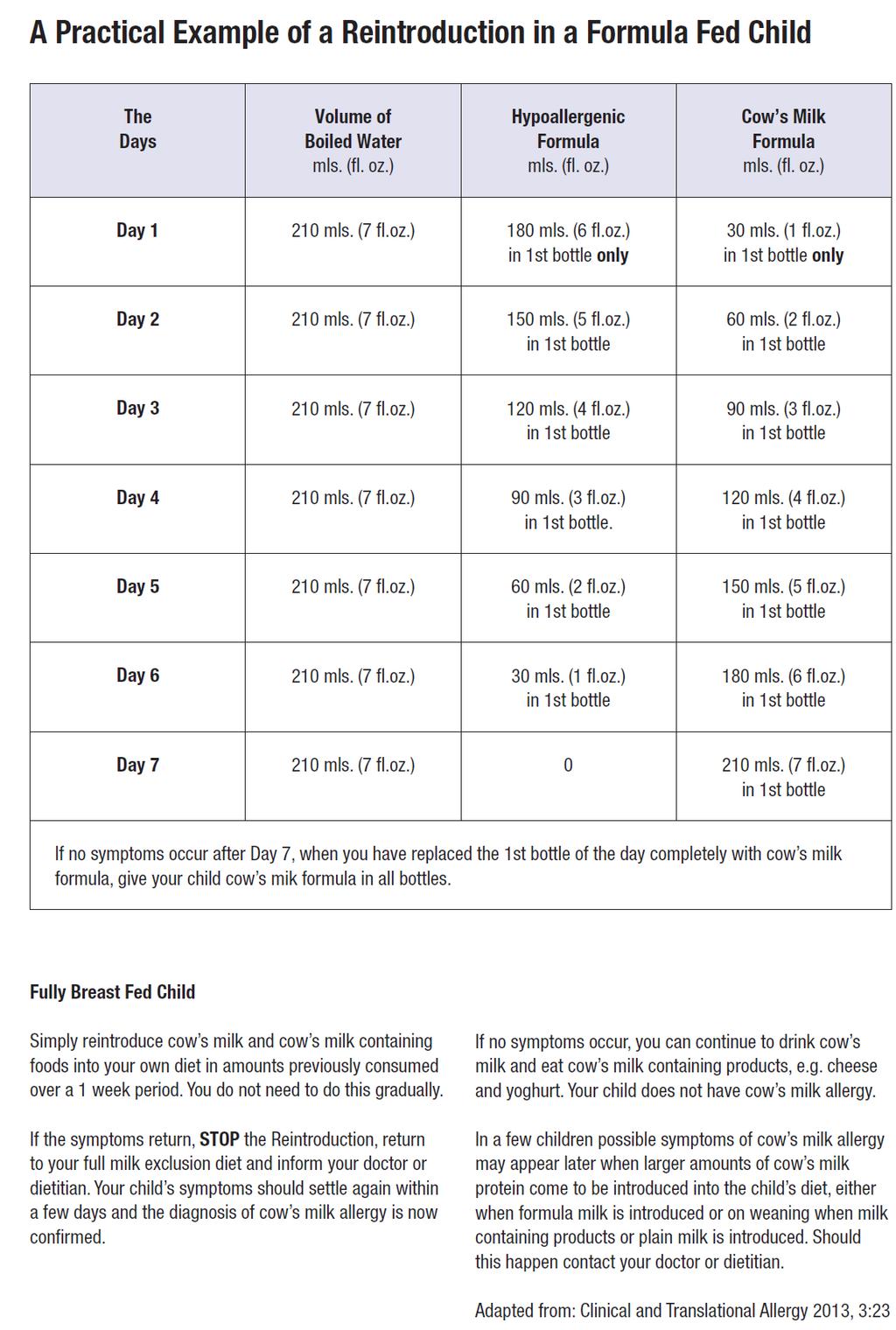
5 3.2.2 Non-IgE mediated CMPA (symptoms onset 2-72hrs) and Home Reintroduction Delayed Onset symptoms: Non-IgE mediated Mild to moderate Several of the following symptoms: vomiting, reflux, loose/ frequent stools, constipation, colic, blood +/- mucus in stools, rhinitis, wheeze, cough, pruritus, erythema, moderate persistant atopic dermatitis. Severe Severe, persisting symptoms of more than one of the following: vomiting, diarrhoea, +/- faltering growth, significant blood +/- mucus in stools, severe atopic dermatitis Mixed/ formula feeding Formula fed: Trial EHf; mixed feeding: CM free maternal diet* + EHf top-ups if needed. Refer to dietitians. Exclusively breastfed CM free maternal diet* for 2-4 weeks. AAf may be advised if top-ups needed. Non-urgent referral to dietitians for weaning advice. Improvement in 2-4 weeks Improvement in 2-4 weeks Yes No Yes No Mixed/ formula feeding** Urgent referral to paediatric allergy service. Exclusive formula feeding: Specialist to commence or recommend AAf. Mixed feeding: Maternal dairy free diet and AAf for faltering growth. Refer to dietitians. Exclusively breastfed** Urgent referral to paediatric allergy service and dietetians. CM free maternal diet* for 2-4 weeks. AAf may be advised if top-ups needed. Home Reintroduction using standard formula to confirm diagnosis, done within 2-4 weeks of elimination diet. Refer to paediatric allergy service for AAf if CMPA still suspected. If not resume normal diet. Home Reintroduction to confirm diagnosis i.e. maternal normal dairy diet for 1-2weeks, after 2-4 weeks of dairy exclusion. Refer to paediatric allergy service if CMPA still suspected. If not resume normal maternal diet. Symptoms return Resume EHf and if symptoms return - CMA now confirmed. No return of symptoms Not CMPA Symptoms return Resume maternal dairy free diet and if symptoms settle - CMPA confirmed. AAf top ups can be maintained if no weight gain concerns. Refer to specialist for faltering growth and persistent symptoms. No return of symptoms Not CMPA * Breastfeeding mothers on a milk free diet may require supplementation with 1000mg calcium and 10mcg Vitamin D per day. ** Do not perform Home Reintroduction in those with severe symptoms. AAf = amino acid formula; EHf = extensively hydrolysed formula Early Home Reintroduction to confirm diagnosis - mild-moderate symptoms only EHf should be continued for a minimum of 2 weeks and if symptoms have improved, it is vital that parents perform Home Reintroduction after 2-4 weeks of starting EHf, in order to confirm the diagnosis. If symptoms return, CMPA is confirmed and EHf should be resumed. If symptoms do no return with the Home Reintroduction, CMPA is ruled out. How the Reintroduction is carried out is dependent on whether the infant is exclusively breastfed or mixed/ bottle-fed. imap s parent leaflet on The Early Home Reintroduction to confirm diagnosis can be downloaded to share with parents (see appendix 4). 5
6 3.3 Ongoing Management of Confirmed Mild to Moderate CMPA Confirmed Mild-moderate CMPA Exclusively breast-fed Marternal dairy free diet* + AAf as advised by specialist if needed as top-ups. Or Mixed/ formula fed Continue EHf; or AAf as per advice from secondary care if intolerant to EHf Non-IgE mediated IgE mediated No current atopic dermatitis and no history at any stage of acute onset symptoms. Home Reintroduction with support from health visitors or dietitians as per imap ladder. * Breastfeeding mothers on a milk free diet may require supplementation with 1000mg calcium and 10mcg Vitamin D per day. AAf = amino acid formula; EHf = extensively hydrolysed formula 3.4 Product Choices Extensively Hydrolysed Formula (EHf) EHf is the first line treatment for mild to moderate CMPA in primary care. These formulas are tolerated by 90% of infants with CMPA. There is emerging evidence that tolerance to cow s milk occurs sooner on sustained exposure to EHf, so early diagnosis and a switch from standard formula to EHf will eliminate allergen sooner, improve symptoms control and could facilitate natural resolution of CMPA. Traffic Light CM free diet for at least 6 months and until 9-12 months of age (with weaning support from dietitians). Test for acquired tolerance depending on status of atopic dermatitis and history of acute onset symptoms. Current atopic dermatitis during CM free diet Allergy clinic for IgE testing or skin prick test Negative and no history at any stage of acute onset symptoms. History of acute onset symptoms at any time. Allergy clinic for IgE testing or skin prick Positive Refer to specialist paediatritian, may need supervised challenge. Follow up with serial IgE testing and later planned and Supervised Challenge in secondary care or specialist setting to test for acquired tolerance. Dietietic referral required. Negative Liaise with paediatric allergy service regarding re-challenge. Product Age group Notes Cost/ 100g (June 2017) EHf 1st line choices for mild to moderate CMPA Similac From birth Most cost-effective EHf. Lactose free Alimentum Althera From birth Contains lactose. May be used where 2.37 gastrointestinal symptoms are not present, or if there is a palatability issue. Aptamil Pepti 1 From birth 6 Contains lactose. May be used where 2.47 Aptamil Pepti 2 months Over 6 months gastrointestinal symptoms are not present, or if there is a palatability issue
7 Traffic Light Product Age group Notes Cost/ 100g (June 2017) Nutramigen 1 From birth 6 Lactose free. Contains a unique 2.75 with LGG Nutramigen 2 with LGG months Over 6 months probiotic Lactobacillus rhamnosus GG (LGG ) EHf with MCT (medium chain triglycerides) Initiated by secondary Care only Pregestimil Lipil From birth Suitable only when CMPA is also 3.05 Pepti Junior From birth accompanied by fat malabsorption NB: Infatrini Peptisorb is a high calorie EHf for mild to moderate CMPA with poor intake and poor weight gain but no significant growth faltering. See also section Amino Acid Formula (AAf) In AAf, the milk protein is broken down into individual amino acids. AAf is suitable only if at least one of the following criteria is met: Persistent symptoms after 4 weeks on EHf; Severe CMPA such as faltering growth and severe GI symptoms; A history of anaphylactic reaction to cow s milk formula; Persistent symptoms in breast fed infants unresponsive to maternal dairy free diet for 4 weeks, or mother does not wish to continue breastfeeding. AAf should only be prescribed on advice or recommendation of a Paediatric Consultant. GPs can contact the consultant-led paediatric allergy advice service via oxon.paedsallergyadvice@nhs.net for specialist advice on appropriateness of AAf before starting it in new patients. Traffic Light Product Age group Notes Cost/ 100g (June 2017) AAf Secondary Care Recommendation/ Initiation only Alfamino From birth up to 18 months old, or when able to tolerate OTC products Nutramigen PurAmino Most cost-effective AAf. Has higher vitamin A content. Gluten and lactose free. Previously known as Nutramigen AA. Neocate LCP From birth - 1 year Can be used as a sole source of nutrition up to the age of 1 year. Other AAf Neocate Junior From 1 year 10 years Neocate Junior will replace Neocate Active and Neocate Advance over a period of 12 months, from April 2017 to April These are high calorie formulas and will not be required automatically by all infants over 1 year. Suitable as a sole source of nutrition or as a supplement (unflavoured / vanilla/ strawberry) 7
8 3.4.3 Products Not Suitable for Prescribing in CMPA 1. Soya products: Wysoy Soya products should NOT be routinely prescribed for infants with CMPA, in particularly those under 6 months due to high phytoestrogen content. It may be used in infants over 6 months who do not tolerate first line EHf due to issues with palatability. There is a risk of co-sensitisation to soya in infants with predominantly GI symptoms of CMPA. It is more likely that children will tolerate soya formula from 1 year, and parents should be advised to purchase soya formula or Alpro Soya Growing Up Drink (1+ Years) from 1 year of age as these are similar costs to cow s milk formula, in line with Clinical Commissioning Policy 88 and Lactose free formula: Aptamil LF, SMA LF and Enfamil O-Lac. Lactose intolerance is not the same as CMPA and these formulas are cow s milk based. EHf or AAf should not be prescribed for transient lactose intolerance. 3. Rice milk: Unsuitable under age of 5yrs due to arsenic content. 4. Other mammalians milk e.g. Goat milk, Sheep milk products have similar protein composition to cow s milk so are not suitable for treating CMPA. 3.5 Prescription Management 1. Try a formula for a minimum of two weeks and maintain for at least four weeks before further changes. 2. Specialist formulas may be prescribed for infants with CMPA usually for no longer than 6 12 months. All children on EHf should be reviewed by GPs at 12 months and then 18 months as appropriate. For those who are on AAf, GPs should review latest correspondence from the specialist or dietitian as there may be changes in formula or quantity. 3. Parents of all children with non-ige CMPA should be advised on graded dairy introduction using the imap milk ladder (see appendix 5) after 6 months of exclusion. This is a test for acquired tolerance and helps resolution if certain dairy products are well tolerated. The imap milk ladder (see appendix 5) should be shared with parents as it contains useful practical pointers to support parents at home. imap milk ladder recipes can be downloaded here. 4. Review prescriptions regularly and refer to latest correspondence from specialist for any change in formula or quantity. Review and consider stopping prescription if the patient meets one or more of the following criteria: On the formula for more than a year The quantity of formula prescribed is higher than recommended above (see section 2.1) Patient can eat cow s milk containing foods such as cow s milk, cheese, yogurt, ice-cream, custard, cakes, chocolate, cream, ghee and etc. Over 18 months old. Please note children with multiple or severe allergies may require prescriptions beyond 18 months old. This should always be on the recommendation of the paediatric dietitian or consultant. 8
9 Please send a new referral or liaise with appropriate services if the child is already under the care of a paediatric dietitian or paediatric allergist. 3.6 Reintroducing Cow s Milk Products 1. Note that this is different from the Early Home Reintroduction usually performed 2 4 weeks after introducing EHf, which is aimed at confirming CMPA diagnosis (see section 3.2.2). 2. Children on long-term EHf or AAf should be reintroduced to dairy on a graded approach, to establish if they have acquired tolerance to CMP. About 60 75% of children outgrow CMPA by 2 years of age, rising to 85-90% at 3 years of age. 3. For exclusively breastfed infants who have been symptom-free for at least 6 months: - Re-introduce dairy products to maternal diet from 9-12 months and if tolerated, use the imap milk ladder (see appendix 5) for graded dairy re-introduction. imap milk ladder recipes can be downloaded here. 4. For formula only and mixed formula/ breast-fed children who have been symptom-free for at least 6 months: - Re-introduce cow s milk products using the the imap milk ladder (see appendix 5) around 9-12 months old and every 2 months thereafter until tolerated. imap milk ladder recipes can be downloaded here. 5. All children with IgE CMPA should have a plan of dairy reintroduction from Paediatric allergist when safe. No Home Reintroductions should be performed in these patients. 3.7 Weaning When an infant with CMPA reaches 6 months and starts to be weaned, it is important that an adequate calcium intake is achieved, particularly whilst remaining on a CM-free weaning diet. Refer to community or paediatric dietitian for support at this stage. 9
10 4. Gastro-oesophageal Reflux Disease (GORD) GORD is the passage of gastric contents into the oesophagus causing troublesome symptoms and/ or complications. About 50% of infants have some degree of reflux at some time. In most infants it is physiological and with minimal effect so most parents can be reassured. Regurgitation of feeds is worse with higher volumes of feed but improves with thickened feeds. Symptoms: effortless vomiting after feeding (not projectile) usually in the first 6 months e.g. regurgitation of a significant volume of feed, reluctance to feed, distress/ crying at feed times, small volumes of feed being taken Does the infant have faltering growth? No Rule out over feeding: check volume and frequency of feeds - average requirement in babies <6 months is 150ml/kg/day and should be spread over 6-7 feeds. Advise on feeding position and activity following a feed. The infant is thriving BUT distressed Bottlefed Trial using Carobel to thicken standard formula or one of the following for 1-2 weeks. These are available OTC and should be purchased by parents: Cow and Gate Anti-reflux, Aptamil Anti-reflux, SMA Staydown, SMA PRO Anti-reflux, Enfamil AR. If symptoms persist, STOP the thickening formula and trial Infant Gaviscon for 1-2 weeks. DO NOT prescribe separate thickeners, antacids, PPIs or ranitidine with thickening formula. Yes Yes The infant is thriving and NOT distressed Refer to specialist paediatric Breastfed Trial with Infant Gaviscon offered on a spoon for 1-2 weeks, up to max 6 times a day Review Improvement If infant is clearly overfed, advise restriction of volumes of feed Reassure and monitor, symptoms are likely to improve over time, usually by 12 months. Provide advice on avoidance of overfeeding, positioning during and after feeding, and activity after feeding. No improvement Refer to specialist paediatrician care Continue with treatment and review regularly to check growth and symptoms. Trial stopping treatment at intervals and by 12 months as 90% of children usually outgrow GORD by then. Once vomiting resolves return to standard formula. Traffic Light Product Cow & Gate Antireflux Aptamil Anti-reflux SMA Staydown* SMA PRO Antireflux Age group From birth Notes Readily available to purchase OTC in most pharmacies and major supermarkets. *N/B: SMA Staydown will be available for a further few months (replaced by SMA PRO Anti-reflux). Cost/ 100g (June 2017) 1.28 (R*) 1.44 (R) 1.22 (R) 1.25 (R) R* = Retail price Enfamil AR This may need to be ordered in specially at the pharmacy 1.73 (R) 10
11 5. Secondary Lactose Intolerance Primary lactose intolerance is rare and is caused by an inherited deficiency of lactase which breaks down lactose. Primary lactase deficiency usually develops after the age of two years, when breastfeeding or bottle-feeding has stopped. The symptoms may not be noticeable until adulthood. Secondary lactose intolerance is due to impaired lactase activity in the intestinal brush border and it is neither immune mediated nor a feature of atopy. Secondary lactose intolerance in children occurs post gastroenteritis and rarely following other gut insults such as prolonged courses of antibiotics. Symptoms are usually self-limiting. Parents of breastfed babies with lactose intolerance should be advised to purchase lactase enzyme drops (e.g. Colief ). This should not be prescribed on the NHS. Exclusion of lactose from the maternal diet is unnecessary as lactose is present in breast milk independent of diet. More severe or persistent symptoms suggestive of lactose intolerance will need paediatric assessment if lactase is ineffective. Alternative diagnosis such as CMPA will need to be considered for persistent gastrointestinal symptoms. Parents qualifying for Healthy Start vouchers can use these to purchase lactose free formula where the packaging states that the milk is based on cow s milk and can be used from birth, e.g. SMA LF and Enfamil O-Lac. Symptoms: abdominal bloating, increased (explosive) wind, loose green stools for > 2 weeks. Diagnosis is confirmed if symptoms resolved within 48 hours of withdrawing lactose from diet. Trial OTC lactose-free formula for 2 weeks. These can be bought at a similar cost to standard formula: <12 months: Aptamil LF, SMA LF, Enfamil O-Lac (may need to pre-order from pharmacies) >12 months: LF full fat milk (e.g. Lactofree brand) can be bought in supermarkets Symptoms improved Symptoms not improved Lactose Intolerance confirmed Continue LF formula for up to 8 weeks gradually then reintroduce standard formula/milk into diet. If symptoms return restart LF formula until normal dairy tolerated. There is a need to await natural resolution. Referral needed if symptoms do not improve on LF formula. Not lactose Intolerance Consider alternative diagnosis e.g. CMPA. Refer to specialist care. Note: Rarely symptoms may last up to 3 months Traffic Light Product Age group Notes Cost/ 100g (June 2017) Enfamil O- Lac From birth to 1 year Lactose, sucrose and fructose free cow s milk formula. May need to be 2.30 (R*) ordered in specially at the pharmacy. SMA LF From birth up to Not suitable for those who are allergic 1.40 (R) 1 year to cows' milk protein. Available to Aptamil LF From birth to 1 purchase OTC in pharmacies and 1.50 (R) year major supermarkets. Lactofree From 1 year 0.14/ 100ml (R) R* = Retail price 11
12 6. Faltering Growth Faltering growth is when an infant falls below the 0.4 th centile or crosses 2 centiles downwards from initial centile on a growth chart. Refer to paediatric services without delay. Specialist formula for children with faltering growth should only be prescribed in primary care following assessment and recommendations from a Consultant Paediatrician or Paediatric Dietitian. GPs can access specialist advice via oxon.paediatricadvice@nhs.net. Traffic Light Product Age group Notes Cost/ 100ml (June 2017) SMA PRO Refer to 0.99 High Energy From birth up to 18 months or 8kg. paediatric Similac High services without 1.07 Energy Infatrini delay. All infants will need growth 1.16 Infatrini Peptisorb From birth up to 18 months or 9kg. Suitable for infants with faltering growth and intolerance to whole protein feeds, e.g. short bowel syndrome, intractable malabsorption, inflammatory bowel disease, bowel fistulae monitoring to ensure catch up growth is achieved. Discontinue when on an appropriate diet as per dietitian advice Preterm Infants Pre-term infants will have been commenced on a pre-term formula (eg Nutriprem ) in hospital prior to discharge. Pre-term formula should not be commenced in primary care unless recommended by a specialist. The GP can continue prescribing the pre-term formula, until the baby is 6 months corrected age i.e. Expected Delivery Date (EDD) + 26 weeks. At this stage the GP should review the prescription and switch to a standard term formula which should be purchased by parents. If there is a concern about growth, the baby should be referred back to the neonatal unit for advice. Not all babies require pre-term formula for the full 26 weeks from EDD. If there is excessive weight gain at any stage up to 6 months corrected age, the pre-term formula may be discontinued and a change made to a standard formula. Ready to feed liquids are substantially more expensive than the powder and should not be prescribed in primary care unless there is a clinical need e.g. the baby is immunocompromised, tube fed or there has been a specific request by secondary care. Traffic Light Product Age group Notes Cost/ 100 kcals (June 2017) Nutriprem 2 From birth GP to review and stop prescription 0.26 powder SMA PRO Gold Prem 2 powder to 6 months (corrected age) at 6 months corrected age or if excessive weight gain
13 Traffic Light Product Age group Notes Cost/ 100 kcals (June 2017) Nutriprem 2 liquid Only prescribe if the infant is 1.16 SMA PRO Gold Prem 2 liquid immune-compromised, tube fed or as directed by secondary care Metabolic Products Children under Dietetic Care may need to have other specialist formulas for reasons other than CMPA. Two examples of these could include formulas or products for metabolic patients and hydrolysed or amino acid based formulas for gastroenterology symptoms or treatment. 9. References and Acknowledgement References: Bernie Canani R et al. (2013) Formula selection for management of children with cow s milk allergy influences the rate of acquisition of tolerance: a prospective multicentre study. J Pediatr, 163 (3): Buller HA, Rings EH, Montgomery RK,Grand RJ. (1991) Clinical aspects of lactose intolerance in children and adults. Sc and J Gastroenterolgy Suppl,188: Food Standard Agency statement on arsenic levels in rice milk (2009) arsenicinrice.pdf Milk Allergy in Primary Care (MAP) Guidelines: Venter C, Brown T, Shah N, Walsh J Fox AT. (2013) Diagnosis and management of non-ige-mediated cow's milk allergy in infancy - a UK primary care practical guide, Clinical and Translational Allergy, 3:23. Venter et al. (2017) Better recognition, diagnosis and management of non-ige-mediated cow s milk allergy in infancy: imap an international interpretation of the MAP (Milk Allergy in Primary Care) guideline, Clinical Translational Allergy, 7:26. NICE (2011) Food Allergy in Children and Young People. NICE (2015) Gastro-oesophageal reflux disease in children and young people. NG1 Acknowledgement: This guideline has been produced by the Medicines Optimisation Team, Oxfordshire Clinical Commissioning Group in consultation with: Dr Felicitas Obetoh, Paediatrician with Interest in Allergy, Paediatric Allergy Clinic, Oxford University Hospitals NHS Trust 13
14 Dr Kenny McCormick, Neonatal consultant, Oxford Newborn Care Unit, Oxford University Hospitals NHS Trust Katheryn Clarke and colleagues, Community Paediatric Dietetics Team, Oxford University Hospitals NHS Foundation Trust Suzanne Bradshaw, Prescribing Support Dietitian, Oxfordshire Clinical Commissioning Group This guideline has been based on the following documents: PrescQIPP Bulletin 146, November 2016: Appropriate prescribing of specialist infant formulae (foods for special medical purposes) Central London Community Healthcare, Paediatric Dietetics Service, August 2015: Primary Care Specialist Infant Formulae Prescribing Guidance Pan Mersey Area Prescribing Committee, November 2014: Pan-Mersey Prescribing Guidelines for Specialist Infant Formula Feeds in lactose Intolerance and Cow s Milk Protein Allergy. Ipswich and East Suffolk Clinical Commissioning Group, September 2015: Recommendations for Prescribing Specialist Infant Formula 2015/16. 14
 in the 1 st Year of")
15 Appendix 1: Suspected Cow s Milk Allergy (CMA) in the 1 st Year of Life 15

16 Appendix 2: Primary Care Management of Mild to Moderate Non-IgE CMA 16

17 Appendix 3: Initial factsheet for parents 17
18 18

19 Appendix 4: The Early Home Reintroduction to Confirm Diagnosis leaflet for parents 19
20 20

21 Appendix 5: The imap Milk Ladder 21

22 22
23 Appendix 6: Infant Formula products quick reference guide ALL CONDITIONS - Suggested Prescribing Quantities of Powdered Formula per month < 6months 6-12 months >12 months 13 x 400g tin OR 6 x 900g tins 7-13 x 400g tins OR 3-6 x 900g tins 7 x 400g tins OR 3 x 900g tins Milk Type Proprietary Brand Suitable for Cost / Original pack (T = Trade; R = Retail) Cost / 100g or 100ml Supply Route Cow s Milk Protein Allergy (CMPA) Nutramigen LGG1 < 6m (400g)T 2.75 FP10 Extensively Hydrolysed Formula (EHf) Amino Acid Formulas (AAf) Nutramigen LGG2 > 6m (400g) T 2.75 FP10 Aptamil Pepti 1 < 6m (800g) T 2.47 FP10 Aptamil Pepti 2 > 6m 9.35 (400g) T 2.35 FP10 Similac Alimentum 0 18m 9.10 (400g) T 2.28 FP10 Althera 0 18m (450g) T 2.37 FP10 Pregestimil Lipil From birth (400g) T 3.05 FP10 Pepti Junior From birth (450g) T 2.90 FP10 SMA Alfamino From birth (400g) T 5.75 FP10 Nutramigen PurAmino From birth (400g) T 6.77 FP10 Neocate LCP From birth (400g) T 7.18 FP10 Neocate Junior From 1 year to (400g) T 7.18 FP10 years Review need if child is 18 months, has been prescribed for >1 year, able to eat cheese, yoghurt, chocolate, or butter Gastro-oesophageal Reflux Disease Anti-Reflux Cow & Gate Anti-reflux From birth (900g) R 1.28 OTC Aptamil Anti-reflux From birth (900g) R 1.44 OTC *SMA Staydown From birth (900g) R 1.22 OTC SMA PRO Anti-reflux From birth (800g) R 1.25 OTC **Enfamil AR From birth 6.90 (400g) R 1.73 OTC * Being replaced by SMA PRO Anti-reflux and is available for further few months. ** may have to be specially ordered at the pharmacy Secondary Lactose intolerance Lactose-free SMA LF < 12m 6.00 (430g) R 1.40 OTC Enfamil O-Lac < 12m 9.21 (400g) R 2.30 OTC Aptamil LF < 12m 5.99 (400g) R 1.50 OTC Lactofree >12m 1.35 (1000ml) R 0.14 Shops Symptoms usually resolve within 8 weeks. Lactose free milk is available in supermarkets for infants > 12 months Faltering Growth High energy SMA PRO High Energy Birth 18m/ 8kg 1.97 (200ml) T 0.99 FP10 Similac High Energy Birth 18m/ 8kg 2.13 (200ml) T 1.07 FP10 Infatrini Birth 18m/ 8kg 2.23 (200ml) T 1.11 FP10 Infatrini Peptisorb Birth 18m/ 9kg 3.54 (200ml) T 1.77 FP10 Ensure that there is a clear goal and discontinuation point Pre-term Initiated in secondary care Nutriprem 2 powder SMA PRO Gold Prem 2 powder Nutriprem 2 liquid SMA PRO Gold Prem 2 liquid Birth 6m (corrected age) Birth 6m (corrected age) Birth 6m (corrected age) Birth 6m (corrected age) (900g) T 0.26 FP (400g) T 0.23 FP (200ml) T 1.12 FP (250ml) T 1.16 FP10 These milks are not suitable for infants > 6months (corrected age). Do not prescribe ready to use liquid unless essential 23
24 Appendix 7: Summary of guidelines (NOT TO BE USED FOR DIAGNOSIS) Summary of Guidelines on prescribing specialist infant formula in primary care (NOT TO BE USED FOR DIAGNOSIS) For diagnosis and prescribing please see the full OCCG guidelines. Some children may require more, e.g. those with faltering growth. Review recent correspondence from the paediatrician or paediatric dietitian. All conditions: Under 6 months 6 12 months Over 12 months How much powdered infant formula should I prescribe monthly? 400g tin 900g tin 400g tin 900g tin 400g tin 900g tin Up to 12 tins Up to 5 tins 6 12 tins 3 5 tins Up to 6 tins Up to 3 tins IgE symptoms (<2hrs onset) [See page 4 of the full guidelines for diagnosis algorithm] Skin symptoms: urticaria, pruritus, angioedema; respiratory: difficulty in breathing and swallowing, hoarse cry, acute wheeze or anaphylaxis. Non-IgE symptoms (2-72hrs onset) [See page 5 of the full guidelines for diagnosis algorithm] - Skin symptoms: pruritus, erythema, urticaria, atopic dermatitis; GI symptoms: diarrhoea, bloody stools, vomiting, abdominal distention, colicky pain, constipation, GORD; Respiratory symptoms: recurrent wheeze/ cough, nasal itching, sneezing or congestion and rhinorrhoea. Growth faltering. Cow s Milk Protein Allergy (CMPA): Most infants with CMPA develop symptoms within 1-2 weeks of introduction. Mild moderate non-ige CMPA can be managed in primary care. Early diagnosis and treatment is very important. Download The imap Milk Allergy Guideline Initial Fact Sheet for parents whose infants fall under this group. Breast milk is the best choice for most infants with CMPA. Breastfeeding mothers may require a dairy free diet and daily 1000mg calcium and 10 mcg Vitamin D supplementation. Refer to paediatric community or paediatric dietitians for weaning advice before infant is 6 months of age. Always review the latest clinic correspondence before issuing each prescription to ensure any recommended changes are implemented. First line: Extensively Hydrolysed formula (EHf) Most cost-effective: Similac Alimentum Soya milk, lactose-free (LF) formula, rice milk or other mammalians Other options: Althera, Aptamil Pepti 1&2, Nutramigen milk are not suitable in CMPA 1&2 with LGG To confirm diagnosis, perform Early Home Reintroduction in infants with mild-moderate non-ige CMPA (2 72 hours). Not safe for immediate symptoms of IgE CMPA. At diagnosis EHf should be continued for at least 2-4 weeks and if symptoms improve, Home Reintroduction should be performed after 2-4 weeks of starting EHf to confirm the diagnosis of CMPA. Download imap s parent leaflet on The Early Home Reintroduction to confirm diagnosis to support parents at home. Second line: Amino Acid formula (AAf) Secondary care initiation or recommendation only. Consultant-led advice: oxon.paedsallergyadvice@nhs.net. Refer infants with anaphylaxis or faltering growth to secondary care urgently. Most cost-effective: Alfamino Other options: Nutramigen PurAmino, Neocate LCP, Neocate Junior Reintroduction: Patients should be evaluated after at least six months of exclusion of dairy products to assess acquired tolerance to CMP. Download imap milk ladder and recipes to support parents reintroduce CM at home, provided there is no history of immediate allergic reactions or other indications for referral to secondary care. Review the need for specialised formula prescription regularly and consider STOPPING if any of the following applies: Can the patient tolerate any dairy foods? Is the patient over 18 months old (continue treatment if specifically indicated by specialists)? Has the formula been prescribed for more than one year? Is the quantity prescribed more than the recommended amount?
25 Gastrooesophageal Reflux Disease (GORD) Secondary Lactose Intolerance Faltering Growth GORD presents with a history of effortless vomiting after feeding (up to two hours), usually in the first six months of life. [See page 10 of the full guidelines for more details] Over feeding should be ruled out by establishing the volume and frequency of feeds. Give reassurance and advice on positioning post-feeds. Infant Gaviscon can be given up to a maximum of six times per day. Initially recommend adding Carobel (available from pharmacies) to current standard formula, or trial anti-reflux formula (available from pharmacies/ supermarkets) for 1-2 weeks and review symptoms. Cow and Gate Anti-reflux, Aptamil Anti-reflux, SMA PRO Anti-Reflux, Enfamil AR Secondary lactose intolerance usually occurs following an infectious GI illness (but can occur alongside new or undiagnosed coeliac disease) and is usually self-limiting. [See page 11 of the full guidelines for more details] Symptoms include abdominal bloating, increased explosive wind and loose green stools. Resolution of symptoms within 48 hours of withdrawal of lactose from the diet confirms diagnosis. Initially recommend over-the-counter lactose-free (LF) formula for two weeks. Continue LF formula for up to eight weeks if symptoms improved. Symptoms usually resolve within this time but in rare cases may take up to three months months: Enfamil O-Lac, SMA LF, Aptamil LF Over 12 months: Lactofree Faltering growth cannot be detected without using a growth chart. Diagnosis is usually made when an infant falls below the 0.4th centile or crosses 2 centiles downwards on a weight or height centile. [See page 12 of the full guidelines for more details] Consultant-led advice: oxon.paediatricadvice@nhs.net. First line: High-energy formula Secondary care initiation or recommendation only. Discontinue when on an appropriate diet as per dietitian advice. Refer infants with faltering growth to secondary care without delay. Refer to secondary care without delay. Most cost-effective: SMA PRO High Energy Other options: Similac High Energy, Infatrini, Infatrini Peptisorb (high calorie EHf) These infants will have had their pre-term formula commenced on discharge from the neonatal unit and will be under regular review by the paediatricians. Pre-term formula should not be commenced in primary care unless recommended by a specialist. GPs should discontinue these formulas after the infants are six months corrected age or if there is excessive weight gain. [See page 12 of Pre-term the full guidelines for more details] Started in secondary care: Pre-term formula Nutriprem 2 powder, SMA PRO Gold Prem 2 powder DO NOT prescribe liquid formula unless immune-compromised, tube Nutriprem 2 liquid, SMA PRO Gold Prem 2 liquid fed or clinically indicated by secondary care. This quick reference guide has been adapted from PrescQipp B146: Specialist infant feeds quick reference guide. 25
Prescribing Commissioning Policy May Diagnosis and management of Cow s Milk Protein Allergy (CMPA) and Lactose Intolerance
 and Lactose Intolerance") Prescribing Commissioning Policy May 2018 Diagnosis and management of Cow s Milk Protein Allergy (CMPA) and Lactose Intolerance NHS Eastern Cheshire, NHS South Cheshire and NHS Vale Royal Clinical Commissioning
Prescribing Commissioning Policy May 2018 Diagnosis and management of Cow s Milk Protein Allergy (CMPA) and Lactose Intolerance NHS Eastern Cheshire, NHS South Cheshire and NHS Vale Royal Clinical Commissioning
GP Patient Pathway for Infants under 1 year of age with Cows Milk Protein Allergy (Non IgE Mediated)
") GP Patient Pathway for Infants under 1 year of age with Cows Milk Protein Allergy (Non IgE Mediated) Infant suspected with (non IgE) after an allergy focused clinical history has been completed (see appendix
GP Patient Pathway for Infants under 1 year of age with Cows Milk Protein Allergy (Non IgE Mediated) Infant suspected with (non IgE) after an allergy focused clinical history has been completed (see appendix
COW S MILK PROTEIN ALLERGY IN CHILDREN
 COW S MILK PROTEIN ALLERGY IN CHILDREN Wednesday 8th June 2016 By Dr Rukhsana Hussain CMPA Cows' milk protein allergy is an immune-mediated allergic response to proteins in milk Milk contains casein and
COW S MILK PROTEIN ALLERGY IN CHILDREN Wednesday 8th June 2016 By Dr Rukhsana Hussain CMPA Cows' milk protein allergy is an immune-mediated allergic response to proteins in milk Milk contains casein and
Guideline for Prescribing Specialist Infant Formula in Primary Care For Infants With Cow s Milk Protein Allergy (CMPA) or Lactose Intolerance
 or Lactose Intolerance") Guideline for Prescribing Specialist Infant in Primary Care For Infants With Cow s Milk Protein Allergy (CMPA) or Lactose Intolerance Date Produced: March 2013 Date for Review: March 2015 Version: 2.0
Guideline for Prescribing Specialist Infant in Primary Care For Infants With Cow s Milk Protein Allergy (CMPA) or Lactose Intolerance Date Produced: March 2013 Date for Review: March 2015 Version: 2.0
Dietary Management of Cow s Milk Protein Allergy
 Dietary Management of Cow s Milk Protein Allergy Amy Roberts Paediatric Dietitians September 2014 Objectives To increase confidence in diagnosing a cow s milk allergy To understand the difference between
Dietary Management of Cow s Milk Protein Allergy Amy Roberts Paediatric Dietitians September 2014 Objectives To increase confidence in diagnosing a cow s milk allergy To understand the difference between
Hertfordshire Guidelines for Specialist Infant Feeds - CMPA - (HMMC) Feb 2015 (Updated July 2015 and June 2016)
 Feb 2015 (Updated July 2015 and June 2016)") COWS MILK PROTEIN ALLERGY (CMPA) Symptoms and Diagnosis Refer to NICE Clinical Guideline 116 (February 2011) Food Allergy in children and young people for full details of symptoms, an allergy focused clinical
COWS MILK PROTEIN ALLERGY (CMPA) Symptoms and Diagnosis Refer to NICE Clinical Guideline 116 (February 2011) Food Allergy in children and young people for full details of symptoms, an allergy focused clinical
Prescribing Guidelines for Lactose Intolerance and Cow s Milk Protein Allergy
 Prescribing Guidelines for and Aim To clarify which products and in which circumstances milk substitutes can be prescribed for babies and young children in primary care, as well as to give a guide to prescribing
Prescribing Guidelines for and Aim To clarify which products and in which circumstances milk substitutes can be prescribed for babies and young children in primary care, as well as to give a guide to prescribing
UPDATE ON SPECIALIST INFANT FEEDING GUIDELINES
 UPDATE ON SPECIALIST INFANT FEEDING GUIDELINES Miranda Potter and Lindsey Mowles Specialist Paediatric Dietitians Ipswich Hospital OUTLINE Summary of Specialist Infant Formula Prescribing guidelines Updated
UPDATE ON SPECIALIST INFANT FEEDING GUIDELINES Miranda Potter and Lindsey Mowles Specialist Paediatric Dietitians Ipswich Hospital OUTLINE Summary of Specialist Infant Formula Prescribing guidelines Updated
GUIDANCE ON THE DIAGNOSIS AND MANAGEMENT OF LACTOSE INTOLERANCE AND PRESCRIPTION OF LOW LACTOSE INFANT FORMULA.
 GUIDANCE ON THE DIAGNOSIS AND MANAGEMENT OF LACTOSE INTOLERANCE AND PRESCRIPTION OF LOW LACTOSE INFANT FORMULA. These are the lactose intolerance guidelines and it is recommended that they are used in
GUIDANCE ON THE DIAGNOSIS AND MANAGEMENT OF LACTOSE INTOLERANCE AND PRESCRIPTION OF LOW LACTOSE INFANT FORMULA. These are the lactose intolerance guidelines and it is recommended that they are used in
GUIDANCE ON THE DIAGNOSIS AND MANAGEMENT OF LACTOSE INTOLERANCE
 GUIDANCE ON THE DIAGNOSIS AND MANAGEMENT OF LACTOSE INTOLERANCE These are the lactose intolerance guidelines and it is recommended that they are used in conjunction with the Cow s Milk Allergy guidance.
GUIDANCE ON THE DIAGNOSIS AND MANAGEMENT OF LACTOSE INTOLERANCE These are the lactose intolerance guidelines and it is recommended that they are used in conjunction with the Cow s Milk Allergy guidance.
Prescribing Guidelines for Specialist Infant Formula Feeds
 Prescribing Guidelines for Specialist Infant Formula Feeds Midlands and Lancashire CSU. Contributors to the document: Carol Pinder, Lancashire Teaching Hospitals NHS Foundation Trust (Original version
Prescribing Guidelines for Specialist Infant Formula Feeds Midlands and Lancashire CSU. Contributors to the document: Carol Pinder, Lancashire Teaching Hospitals NHS Foundation Trust (Original version
Guidance On Prescribing Cow's Milk Free Formulae To Treat Cow's Milk Protein Allergy In Infants And Children. Uncontrolled when printed.
 NHS Grampian Guidance On Prescribing Cow's Milk Free Formulae To Treat Cow's Milk Protein Allergy In Infants And Children Co-ordinators: Consultation Group: Approver: Dietetic Prescribing NHS Grampian
NHS Grampian Guidance On Prescribing Cow's Milk Free Formulae To Treat Cow's Milk Protein Allergy In Infants And Children Co-ordinators: Consultation Group: Approver: Dietetic Prescribing NHS Grampian
Manufacturer Type of formula Clinical Indication for use. Extensively hydrolysed casein formula (EHF) Lactose free
 Lactose free") GUIDELINES FOR INDICATIONS FOR USING SPECIALISED INFANT FORMULA FOR INFANTS AGED 0-6 MONTHS formula Extensively Nutramigen 1 with LGG First Line Choice 10.99 Mead Johnson Lactose and / or whole protein
GUIDELINES FOR INDICATIONS FOR USING SPECIALISED INFANT FORMULA FOR INFANTS AGED 0-6 MONTHS formula Extensively Nutramigen 1 with LGG First Line Choice 10.99 Mead Johnson Lactose and / or whole protein
Cow's milk protein allergy (CMPA) suspected
 suspected") Background information Patient information Key messages for this pathway When to suspect CMPA Symptoms of CMPA and assessing severity Symptoms of non IgE mediated CMPA Severe CMPA: urgent referral to paediatric
Background information Patient information Key messages for this pathway When to suspect CMPA Symptoms of CMPA and assessing severity Symptoms of non IgE mediated CMPA Severe CMPA: urgent referral to paediatric
Prescribing Specialist Infant Formula For Proven and Suspected Cow s Milk Allergy under the age of 2 years (and older for certain categories)
") Prescribing Specialist Infant Formula For Proven and Suspected Cow s Milk Allergy under the age of 2 years (and older for certain categories) Written by: Heidi Ball, Paediatric Dietitian UHL Emma Jordan,
Prescribing Specialist Infant Formula For Proven and Suspected Cow s Milk Allergy under the age of 2 years (and older for certain categories) Written by: Heidi Ball, Paediatric Dietitian UHL Emma Jordan,
Guidance for prescribers in Primary Care:
 Guidance for prescribers in Primary Care: Pathway for the Management and Treatment of infants with Cows Milk Protein Allergy (CMA) and Lactose Intolerance (LI) Guidelines developed June 2017 Review date
Guidance for prescribers in Primary Care: Pathway for the Management and Treatment of infants with Cows Milk Protein Allergy (CMA) and Lactose Intolerance (LI) Guidelines developed June 2017 Review date
Nutritional Management of Cow s Milk Allergy (CMA) Croydon University Hospital Dietetic Department
 Croydon University Hospital Dietetic Department") Nutritional Management of Cow s Milk Allergy (CMA) Croydon University Hospital Dietetic Department Outline Types of CMA Cow s milk allergy vs. lactose intolerance Nutritional considerations in diagnosing
Nutritional Management of Cow s Milk Allergy (CMA) Croydon University Hospital Dietetic Department Outline Types of CMA Cow s milk allergy vs. lactose intolerance Nutritional considerations in diagnosing
Does my child have a Cow s Milk Allergy?
 This factsheet has been written to help you understand and gain some advice on suspected cow s milk allergy in babies and children. Cow s milk allergy is one of the most common food allergies to affect
This factsheet has been written to help you understand and gain some advice on suspected cow s milk allergy in babies and children. Cow s milk allergy is one of the most common food allergies to affect
CLINICAL AUDIT. Appropriate prescribing of specialised infant formula for cows milk protein allergy
 CLINICAL AUDIT Appropriate prescribing of specialised infant formula for cows milk protein allergy Valid to December 2019 bpac nz better medicin e Background Specialised infant formulae subsidised on the
CLINICAL AUDIT Appropriate prescribing of specialised infant formula for cows milk protein allergy Valid to December 2019 bpac nz better medicin e Background Specialised infant formulae subsidised on the
Guideline for the Management of Children with Egg Allergy and guidance on referral to paediatric allergy clinic
 Guideline for the Management of Children with Egg Allergy and guidance on referral to paediatric allergy clinic Aim and Scope To give guidance on how to identify those children who have egg allergy or
Guideline for the Management of Children with Egg Allergy and guidance on referral to paediatric allergy clinic Aim and Scope To give guidance on how to identify those children who have egg allergy or
Preventing food allergy in higher risk infants: guidance for healthcare professionals
 Preventing food allergy in higher risk infants: guidance for healthcare professionals This information sheet complements current advice from the Scientific Advisory Committee on Nutrition (SACN) and the
Preventing food allergy in higher risk infants: guidance for healthcare professionals This information sheet complements current advice from the Scientific Advisory Committee on Nutrition (SACN) and the
Understanding Food Intolerance and Food Allergy
 Understanding Food Intolerance and Food Allergy There are several different types of sensitivities or adverse reactions to foods. One type is known as a food intolerance ; an example is lactose intolerance.
Understanding Food Intolerance and Food Allergy There are several different types of sensitivities or adverse reactions to foods. One type is known as a food intolerance ; an example is lactose intolerance.
Using the Milk Ladder to re-introduce milk and dairy
 Paediatric Unit information for parents and carers Using the Ladder to re-introduce milk and dairy This leaflet explains what the Ladder is and how to use it. What is the Ladder? The Ladder is an evidence-based
Paediatric Unit information for parents and carers Using the Ladder to re-introduce milk and dairy This leaflet explains what the Ladder is and how to use it. What is the Ladder? The Ladder is an evidence-based
Pain = allergy surely true?
 Pain = allergy surely true? Dr Warren Hyer Consultant Paediatrician Consultant Paediatric Gastroenterologist Educational objectives Screamers silent reflux is this an internet diagnosis PPI s for abdominal
Pain = allergy surely true? Dr Warren Hyer Consultant Paediatrician Consultant Paediatric Gastroenterologist Educational objectives Screamers silent reflux is this an internet diagnosis PPI s for abdominal
'Every time I eat dairy foods I become ill, could I have a milk allergy.? '. Factors involved in the development of cow's milk allergy:
 'Every time I eat dairy foods I become ill, could I have a milk allergy.? '. Dairy allergy is relatively common in the community. The unpleasant symptoms some people experience after eating dairy foods
'Every time I eat dairy foods I become ill, could I have a milk allergy.? '. Dairy allergy is relatively common in the community. The unpleasant symptoms some people experience after eating dairy foods
Paediatric Food Allergy and Intolerance. Abigail Macleod, Associate Specialist, RBH
 Paediatric Food Allergy and Intolerance Abigail Macleod, Associate Specialist, RBH Ig E mediated food allergy Commonest cause of chronic disease in childhood up to 20% children But treatable, manageable
Paediatric Food Allergy and Intolerance Abigail Macleod, Associate Specialist, RBH Ig E mediated food allergy Commonest cause of chronic disease in childhood up to 20% children But treatable, manageable
Diagnosis and assessment of food allergy in children and young people in primary care and community settings
 Diagnosis and assessment of food allergy in children and young people in primary care and community settings Full guideline November 2010 This guideline was developed following the NICE short clinical
Diagnosis and assessment of food allergy in children and young people in primary care and community settings Full guideline November 2010 This guideline was developed following the NICE short clinical
Milk free diet for children with milk allergy
 Patient information Milk free diet for children with milk allergy Introduction This leaflet is for parents and carers of babies and children with a milk allergy. It outlines how the milk allergy can affect
Patient information Milk free diet for children with milk allergy Introduction This leaflet is for parents and carers of babies and children with a milk allergy. It outlines how the milk allergy can affect
Clinical Manifestations and Management of Food Allergy
 Clinical Manifestations and Management of Food Allergy Adrian Sie Consultant in paediatrics, Wishaw General, Lanarkshire April 2013 To do Bring Allergy plan Prevention photo Contents Is it allergy? How
Clinical Manifestations and Management of Food Allergy Adrian Sie Consultant in paediatrics, Wishaw General, Lanarkshire April 2013 To do Bring Allergy plan Prevention photo Contents Is it allergy? How
Sunderland Guidance on Prescribing Gluten Free Products
 Sunderland Guidance on Prescribing Gluten Free Products Gluten free products have ACBS (Advisory Committee on Borderline Substances) approval on the basis that they may be regarded as drugs for the management
Sunderland Guidance on Prescribing Gluten Free Products Gluten free products have ACBS (Advisory Committee on Borderline Substances) approval on the basis that they may be regarded as drugs for the management
Dr Lisa J Waddell, BSc Nutr (Hons), RD, PhD, MBDA, Community Paediatric Allergy Dietitian, Nottingham, UK
, RD, PhD, MBDA, Community Paediatric Allergy Dietitian, Nottingham, UK") A Practical Interpretation of the imap Guideline for Dietitians in the UK Dr Lisa J Waddell, BSc Nutr (Hons), RD, PhD, MBDA, Community Paediatric Allergy Dietitian, Nottingham, UK Cows milk allergy (CMA)
A Practical Interpretation of the imap Guideline for Dietitians in the UK Dr Lisa J Waddell, BSc Nutr (Hons), RD, PhD, MBDA, Community Paediatric Allergy Dietitian, Nottingham, UK Cows milk allergy (CMA)
DIET AND ECZEMA IN CHILDREN
 Many parents look to diet as the cause of their child s eczema or the reason why the eczema is getting worse. People often think that diet is easy to change and that this could help their child. However,
Many parents look to diet as the cause of their child s eczema or the reason why the eczema is getting worse. People often think that diet is easy to change and that this could help their child. However,
Testing for food allergy in children and young people
 Issue date: February 2011 Understanding NICE guidance Information for people who use NHS services Testing for food allergy in children and young people NICE clinical guidelines advise the NHS on caring
Issue date: February 2011 Understanding NICE guidance Information for people who use NHS services Testing for food allergy in children and young people NICE clinical guidelines advise the NHS on caring
Pediatric Food Allergies: Physician and Parent. Robert Anderson MD Rachel Anderson Syracuse, NY March 3, 2018
 Pediatric Food Allergies: Physician and Parent Robert Anderson MD Rachel Anderson Syracuse, NY March 3, 2018 Learning Objectives Identify risk factors for food allergies Identify clinical manifestations
Pediatric Food Allergies: Physician and Parent Robert Anderson MD Rachel Anderson Syracuse, NY March 3, 2018 Learning Objectives Identify risk factors for food allergies Identify clinical manifestations
What should I do if I think my child needs to follow a dairy free diet?
 pg. 1 pg. 2 Feeding Children, a dairy free diet- an at home guide Children may need to follow a dairy free diet for several different reasons. They may have an allergy to the protein in cow s milk, or
pg. 1 pg. 2 Feeding Children, a dairy free diet- an at home guide Children may need to follow a dairy free diet for several different reasons. They may have an allergy to the protein in cow s milk, or
PREVENTION OF FOOD ALLERGY. Dr Kate Swan Dr Claire Stockdale
 PREVENTION OF FOOD ALLERGY Dr Kate Swan Dr Claire Stockdale Objectives To understand: Food allergy phenotypes The role of the skin barrier in sensitisation Early introduction of food as an allergy prevention
PREVENTION OF FOOD ALLERGY Dr Kate Swan Dr Claire Stockdale Objectives To understand: Food allergy phenotypes The role of the skin barrier in sensitisation Early introduction of food as an allergy prevention
Calcium for infants and children
 Calcium for infants and children Nutrition & Dietetics Department Patient information leaflet This leaflet tells you about: The role of calcium and vitamin D in bone health The recommended amounts of calcium
Calcium for infants and children Nutrition & Dietetics Department Patient information leaflet This leaflet tells you about: The role of calcium and vitamin D in bone health The recommended amounts of calcium
Cow s milk protein allergy and. my baby. A parents guide to cow s milk protein allergy
 Cow s milk protein allergy and my baby A parents guide to cow s milk protein allergy Cow s milk protein allergy (CMPA) and my baby Although a diagnosis can bring a sense of relief, it also brings up a
Cow s milk protein allergy and my baby A parents guide to cow s milk protein allergy Cow s milk protein allergy (CMPA) and my baby Although a diagnosis can bring a sense of relief, it also brings up a
Dietary Advice for Lactose Intolerance
 Dietary Advice for Lactose Intolerance What is a lactose intolerance? Lactose intolerance is when you are unable to digest the natural sugars found in milk or formula milk which is made from cows milk.
Dietary Advice for Lactose Intolerance What is a lactose intolerance? Lactose intolerance is when you are unable to digest the natural sugars found in milk or formula milk which is made from cows milk.
APPROACH TO FOOD ALLERGY IN CHILDREN WHY TALK ABOUT FOOD ALLERGY? DISEASES BLAMED ON FOOD ALLERGY ADVERSE REACTIONS TO FOOD OVERVIEW
 APPROACH TO FOOD ALLERGY IN CHILDREN DR MEERA THALAYASINGAM INTERNATIONAL MEDICAL UNIVERSITY RAMSAY SIME DARBY HEALTHCARE MALAYSIA APAPARI WORKSHOP PHNOM PENH CAMBODIA_ 12 TH SEPT 2015 WHY TALK ABOUT FOOD
APPROACH TO FOOD ALLERGY IN CHILDREN DR MEERA THALAYASINGAM INTERNATIONAL MEDICAL UNIVERSITY RAMSAY SIME DARBY HEALTHCARE MALAYSIA APAPARI WORKSHOP PHNOM PENH CAMBODIA_ 12 TH SEPT 2015 WHY TALK ABOUT FOOD
Associate Professor Rohan Ameratunga
 Associate Professor Rohan Ameratunga Adult and Paediatric Clinical Immunologist and Allergist Auckland 9:25-9:45 Preventing Food Allergy Update on Food allergy Associate Professor Rohan Ameratunga Food
Associate Professor Rohan Ameratunga Adult and Paediatric Clinical Immunologist and Allergist Auckland 9:25-9:45 Preventing Food Allergy Update on Food allergy Associate Professor Rohan Ameratunga Food
Guideline for the Prescribing of Gluten Free Products (NUT5)
") Guideline for the Prescribing of Gluten Free Products (NUT5) Author Medicines Optimisation Team, Sunderland CCG Approved by Sunderland Medicines Optimisation and Guideline Group Current Version 2 Published
Guideline for the Prescribing of Gluten Free Products (NUT5) Author Medicines Optimisation Team, Sunderland CCG Approved by Sunderland Medicines Optimisation and Guideline Group Current Version 2 Published
Introducing Milk-Free solids
 Introducing Milk-Free solids This dietary advice sheet gives some general information to help you make the recommended changes to your baby s diet. If you need more detailed advice or if your baby is following
Introducing Milk-Free solids This dietary advice sheet gives some general information to help you make the recommended changes to your baby s diet. If you need more detailed advice or if your baby is following
Food Allergy A buffet of truths and myths
 Food Allergy A buffet of truths and myths Toronto Anaphylaxis Education Group Adelle R. Atkinson M.D. FRCPC Associate Professor of Paediatrics University of Toronto Clinical Immunologist Division of Immunology
Food Allergy A buffet of truths and myths Toronto Anaphylaxis Education Group Adelle R. Atkinson M.D. FRCPC Associate Professor of Paediatrics University of Toronto Clinical Immunologist Division of Immunology
If a patient does not find any formulary option palatable, please refer him/her to the local dietetic service.
 9.4.2 Enteral nutrition See 3Ts Guidelines on community MUST screening, Food First and use of oral nutritional supplements. When introducing enteral nutrition to patients for the first time, prescribe
9.4.2 Enteral nutrition See 3Ts Guidelines on community MUST screening, Food First and use of oral nutritional supplements. When introducing enteral nutrition to patients for the first time, prescribe
Sequoia Education Systems, Inc. 1
 Functional Medicine University s Functional Diagnostic Medicine Program Module 3 * FDMT 527C The Elimination Diet & The Modified Elimination Diet Wayne L. Sodano, D.C., D.A.B.C.I. & Ron Grisanti, D.C.,
Functional Medicine University s Functional Diagnostic Medicine Program Module 3 * FDMT 527C The Elimination Diet & The Modified Elimination Diet Wayne L. Sodano, D.C., D.A.B.C.I. & Ron Grisanti, D.C.,
Food Challenges. Exceptional healthcare, personally delivered
 Food Challenges Exceptional healthcare, personally delivered Introduction You have been referred to the Immunology department to explore your food allergies. This leaflet provides information on allergies
Food Challenges Exceptional healthcare, personally delivered Introduction You have been referred to the Immunology department to explore your food allergies. This leaflet provides information on allergies
Cow s Milk Allergy of the trickier kind
 Cow s Milk Allergy of the trickier kind Declarations Chair of Dietitian Committee ASCIA (Australasian Society for Clinical Immunology and Allergy) Member FSANZ Food Allergy & Intolerance Scientific Advisory
Cow s Milk Allergy of the trickier kind Declarations Chair of Dietitian Committee ASCIA (Australasian Society for Clinical Immunology and Allergy) Member FSANZ Food Allergy & Intolerance Scientific Advisory
GI Allergy and Tolerance. Jon A. Vanderhoof, M.D. Division of Gastroenterology/Nutrition Boston Children s Hospital Harvard Medical School
 GI Allergy and Tolerance Jon A. Vanderhoof, M.D. Division of Gastroenterology/Nutrition Boston Children s Hospital Harvard Medical School Disclosure Medical Advisor- Mead Johnson Nutrition Food Allergy
GI Allergy and Tolerance Jon A. Vanderhoof, M.D. Division of Gastroenterology/Nutrition Boston Children s Hospital Harvard Medical School Disclosure Medical Advisor- Mead Johnson Nutrition Food Allergy
Primary Prevention of Food Allergies
 Primary Prevention of Food Allergies Graham Roberts Professor & Honorary Consultant, Paediatric Allergy and Respiratory Medicine, David Hide Asthma and Allergy Research Centre, Isle of Wight & CES & HDH,
Primary Prevention of Food Allergies Graham Roberts Professor & Honorary Consultant, Paediatric Allergy and Respiratory Medicine, David Hide Asthma and Allergy Research Centre, Isle of Wight & CES & HDH,
Infants and Toddlers: Food Allergies and Food Intolerance
 Infants and Toddlers: Food Allergies and Food Intolerance A Webinar Presented by the Virginia Infant & Toddler Specialist Network and the Fairfax County Office for Children WHAT IS THE DIFFERENCE BETWEEN
Infants and Toddlers: Food Allergies and Food Intolerance A Webinar Presented by the Virginia Infant & Toddler Specialist Network and the Fairfax County Office for Children WHAT IS THE DIFFERENCE BETWEEN
Peanut and Tree Nut allergy
 Peanut and Tree Nut allergy What are peanuts & tree nuts? Peanuts are also called ground nuts, monkey nuts, beer nuts, earth nuts, goober peas, mendelonas and arachis Tree nuts include almond, Brazil,
Peanut and Tree Nut allergy What are peanuts & tree nuts? Peanuts are also called ground nuts, monkey nuts, beer nuts, earth nuts, goober peas, mendelonas and arachis Tree nuts include almond, Brazil,
The speaker had sole editorial control over the content in this slide deck.
 Paediatric Gastro-Allergy Symposium The speaker had sole editorial control over the content in this slide deck. Any views, opinions or recommendations expressed in the slides are solely those of the speaker
Paediatric Gastro-Allergy Symposium The speaker had sole editorial control over the content in this slide deck. Any views, opinions or recommendations expressed in the slides are solely those of the speaker
FEEDING THE ALLERGIC CHILD
 FEEDING THE ALLERGIC CHILD Berber Vlieg-Boerstra, RD PhD Senior research dietitian OLVG, Amsterdam University of Applied Sciences, Groningen Vlieg&Melse Dietitians, Practice for food allergy Disclose NO
FEEDING THE ALLERGIC CHILD Berber Vlieg-Boerstra, RD PhD Senior research dietitian OLVG, Amsterdam University of Applied Sciences, Groningen Vlieg&Melse Dietitians, Practice for food allergy Disclose NO
Last review date: 07/18 Next review: 07/21 Version 11 1
 The information in this factsheet has been written to help people understand more about egg allergy. Eggs are one of the most common foods to trigger allergic symptoms in babies and young children. Most
The information in this factsheet has been written to help people understand more about egg allergy. Eggs are one of the most common foods to trigger allergic symptoms in babies and young children. Most
Case Study: An approach to managing food allergies in a child
 SASPEN Case Study: An approach to managing food allergies in a child Case Study: An approach to managing food allergies in a child Mrs Shihaam Cader, Chief Dietitian, Red Cross War Memorial Children s
SASPEN Case Study: An approach to managing food allergies in a child Case Study: An approach to managing food allergies in a child Mrs Shihaam Cader, Chief Dietitian, Red Cross War Memorial Children s
FPIES ANOTHER DISEASE ABOUT WHICH YOU SHOULD KNOW OBJECTIVES FPIES FPIES 11/10/2016. What is that? Robert P. Dillard, M.D.
 ANOTHER DISEASE ABOUT WHICH YOU SHOULD KNOW What is that? Robert P. Dillard, M.D. Food Protein Induced Enterocolitis Syndrome. OBJECTIVES 1: Awareness of this syndrome 2: Characteristics 3: Diagnosis 4:
ANOTHER DISEASE ABOUT WHICH YOU SHOULD KNOW What is that? Robert P. Dillard, M.D. Food Protein Induced Enterocolitis Syndrome. OBJECTIVES 1: Awareness of this syndrome 2: Characteristics 3: Diagnosis 4:
1 in 5. In Singapore, allergies like atopic dermatitis (eczema) now affect around. Read on to find out more about allergies.
 now affect around. Read on to find out more about allergies.") In Singapore, allergies like atopic dermatitis (eczema) now affect around 1 in 5 1 Read on to find out more about allergies. Reviewed by Reference: 1. Tan T, et al. Prevalence of allergy-related symptoms
In Singapore, allergies like atopic dermatitis (eczema) now affect around 1 in 5 1 Read on to find out more about allergies. Reviewed by Reference: 1. Tan T, et al. Prevalence of allergy-related symptoms
St.Werburgh s Park Nursery School. Food Policy
 St.Werburgh s Park Nursery School Food Policy Food Policy Policy Context: Healthy eating is essential for families. The school provides a range of activities to improve families diets. Snack times are
St.Werburgh s Park Nursery School Food Policy Food Policy Policy Context: Healthy eating is essential for families. The school provides a range of activities to improve families diets. Snack times are
Beth Strong, RN, FNP-C The Jaffe Food Allergy Institute Mount Sinai School of Medicine New York 2/23/13
 Beth Strong, RN, FNP-C The Jaffe Food Allergy Institute Mount Sinai School of Medicine New York 2/23/13 I do not have any financial disclosure to report Why Challenge? To confirm that the suspected food
Beth Strong, RN, FNP-C The Jaffe Food Allergy Institute Mount Sinai School of Medicine New York 2/23/13 I do not have any financial disclosure to report Why Challenge? To confirm that the suspected food
Allergies and Intolerances Policy
 Allergies and Intolerances Policy 2016 2018 This policy should be read in conjunction with the following documents: Policy for SEND/Additional Needs Safeguarding & Child Protection Policy Keeping Children
Allergies and Intolerances Policy 2016 2018 This policy should be read in conjunction with the following documents: Policy for SEND/Additional Needs Safeguarding & Child Protection Policy Keeping Children
Cow`s Milk Protein Allergy. COW`s MILK PROTEIN ALLERGY Eyad Altamimi, MD
 Cow`s Milk Protein Allergy COW`s MILK PROTEIN ALLERGY Eyad Altamimi, MD Agenda of the talk Definitions CMPA Epidemiology and Pathogenesis CMPA Diagnosis CMPA Management CMPA prevention Adverse Food Reaction
Cow`s Milk Protein Allergy COW`s MILK PROTEIN ALLERGY Eyad Altamimi, MD Agenda of the talk Definitions CMPA Epidemiology and Pathogenesis CMPA Diagnosis CMPA Management CMPA prevention Adverse Food Reaction
LIVING WITH FOOD ALLERGY
 LIVING WITH FOOD ALLERGY D R J E N N Y H U G H E S C O N S U L T A N T P A E D I A T R I C I A N N O R T H E R N H E A L T H & S O C I A L C A R E T R U S T QUIZ: TRUE / FALSE Customers with food allergies
LIVING WITH FOOD ALLERGY D R J E N N Y H U G H E S C O N S U L T A N T P A E D I A T R I C I A N N O R T H E R N H E A L T H & S O C I A L C A R E T R U S T QUIZ: TRUE / FALSE Customers with food allergies
Cow s Milk Allergy: The Facts
 Cow s Milk Allergy: The Facts This Anaphylaxis Campaign fact sheet will mostly focus on infants and young children with a particular type of cow s milk allergy where the symptoms are immediate; that is,
Cow s Milk Allergy: The Facts This Anaphylaxis Campaign fact sheet will mostly focus on infants and young children with a particular type of cow s milk allergy where the symptoms are immediate; that is,
Allergy and Anaphylaxis Policy
 Statement This policy serves to promote an allergy aware community. At Splash Centre we have recognised the need to adopt a policy on allergies that may be present in the children who attend our centre.
Statement This policy serves to promote an allergy aware community. At Splash Centre we have recognised the need to adopt a policy on allergies that may be present in the children who attend our centre.
Food Intolerance & Expertise SARAH KEOGH CONSULTANT DIETITIAN EATWELL FOOD & NUTRITION
 Food Intolerance & Expertise SARAH KEOGH CONSULTANT DIETITIAN EATWELL FOOD & NUTRITION Food Intolerance & Expertise What is food intolerance? Common food intolerances Why are consumers claiming more food
Food Intolerance & Expertise SARAH KEOGH CONSULTANT DIETITIAN EATWELL FOOD & NUTRITION Food Intolerance & Expertise What is food intolerance? Common food intolerances Why are consumers claiming more food
St. Agnes Catholic Primary School Highett Anaphylaxis Policy
 1. Introduction St. Agnes Catholic Primary School Highett Anaphylaxis Policy This policy has been prepared to assist in preventing life threatening anaphylaxis and is based on advice from the Australasian
1. Introduction St. Agnes Catholic Primary School Highett Anaphylaxis Policy This policy has been prepared to assist in preventing life threatening anaphylaxis and is based on advice from the Australasian
Egg ladder for egg reintroduction at home
 Egg ladder for egg reintroduction at home Allergy and Immunology Awareness Program (AIAP) for more informations, please contact the Allergy and Immunology Awareness Program (AIAP): AIAP@hamad.qa http://aiap.hamad.qa
Egg ladder for egg reintroduction at home Allergy and Immunology Awareness Program (AIAP) for more informations, please contact the Allergy and Immunology Awareness Program (AIAP): AIAP@hamad.qa http://aiap.hamad.qa
Symptoms of a mild to moderate allergic reaction can include: swelling of the lips, face and eyes hives or welts abdominal pain and/or vomiting.
 ANAPHYLAXIS POLICY Definition: Anaphylaxis is a severe, rapidly progressive allergic reaction that is life threatening. The most common allergens in school aged children are peanuts, eggs, tree nuts (e.g.
ANAPHYLAXIS POLICY Definition: Anaphylaxis is a severe, rapidly progressive allergic reaction that is life threatening. The most common allergens in school aged children are peanuts, eggs, tree nuts (e.g.
Food Allergy Clinical Update
 Food Allergy Clinical Update This Clinical Update complements ASCIA food allergy e-training for health professionals. The main purpose of this document is to provide an evidence-based, quick reference
Food Allergy Clinical Update This Clinical Update complements ASCIA food allergy e-training for health professionals. The main purpose of this document is to provide an evidence-based, quick reference
The speaker had sole editorial control over the content in this slide deck.
 Paediatric Food Allergy Symposium The speaker had sole editorial control over the content in this slide deck. Any views, opinions or recommendations expressed in the slides are solely those of the speaker
Paediatric Food Allergy Symposium The speaker had sole editorial control over the content in this slide deck. Any views, opinions or recommendations expressed in the slides are solely those of the speaker
Gluten Free Prescribing. Engagement Survey Report Summer 2016
 Gluten Free Prescribing Engagement Survey Report Summer 2016 Background Coeliac disease is an autoimmune disease which is triggered by ingesting gluten. The symptoms vary between individuals and there
Gluten Free Prescribing Engagement Survey Report Summer 2016 Background Coeliac disease is an autoimmune disease which is triggered by ingesting gluten. The symptoms vary between individuals and there
CYANS recommendations for the diagnosis and management of food allergy in children and young people Issue date: 2013
 Children and Young People s Allergy Network Scotland (CYANS) CYANS recommendations for the diagnosis and management of food allergy in children and young people Issue date: 2013 1.Diagnosis of food allergy
Children and Young People s Allergy Network Scotland (CYANS) CYANS recommendations for the diagnosis and management of food allergy in children and young people Issue date: 2013 1.Diagnosis of food allergy
Melbourne University Sport Anaphylaxis Policy
 Melbourne University Sport Anaphylaxis Policy The safety and well-being of children is of prime importance at Melbourne University Sport Programs. All reasonable steps will be taken to ensure the safety
Melbourne University Sport Anaphylaxis Policy The safety and well-being of children is of prime importance at Melbourne University Sport Programs. All reasonable steps will be taken to ensure the safety
: Sumadiono, dr SpA(K) Place/date of birth : Nganjuk, : Staff of Pediatric Dept.UGM Yogyakarta
 Place/date of birth : Nganjuk, : Staff of Pediatric Dept.UGM Yogyakarta") CURRICULUM VITAE Name : Sumadiono, dr SpA(K) Place/date of birth : Nganjuk, 9-10-1956 Occupation : Staff of Pediatric Dept.UGM Yogyakarta Educations : General Doctor : Fac. Of Medicine Unair, Surabaya,
CURRICULUM VITAE Name : Sumadiono, dr SpA(K) Place/date of birth : Nganjuk, 9-10-1956 Occupation : Staff of Pediatric Dept.UGM Yogyakarta Educations : General Doctor : Fac. Of Medicine Unair, Surabaya,
Dietary management of food allergy & intolerance
 Dietary management of food allergy & intolerance Dr Emilia Vassilopoulou BsC, PhD, Post-Doc Clinical Nutritionist Dietitian Food Allergy An adverse immune response to a food protein Reactions to a food
Dietary management of food allergy & intolerance Dr Emilia Vassilopoulou BsC, PhD, Post-Doc Clinical Nutritionist Dietitian Food Allergy An adverse immune response to a food protein Reactions to a food
Anaphylaxis Policy. The symptoms of anaphylaxis can develop quickly although the initial presentation can be delayed and/or mild.
 Anaphylaxis Policy Anaphylaxis is a serious allergic reaction and can be life threatening. The allergic reaction may be related to food, insect stings, medicine, latex, exercise, etc., with the most common
Anaphylaxis Policy Anaphylaxis is a serious allergic reaction and can be life threatening. The allergic reaction may be related to food, insect stings, medicine, latex, exercise, etc., with the most common
Aquarium of the Pacific Food Allergy and Anaphylaxis Protocol
 Aquarium of the Pacific Food Allergy and Anaphylaxis Protocol Purpose Statement: The Aquarium of the Pacific recognizes the increasing prevalence of allergies in children, including many life threatening
Aquarium of the Pacific Food Allergy and Anaphylaxis Protocol Purpose Statement: The Aquarium of the Pacific recognizes the increasing prevalence of allergies in children, including many life threatening
Allergy Awareness and Management Policy
 Allergy Awareness and Management Policy Overview This policy is concerned with a whole school approach to the health care management of those members of our school community suffering from specific allergies.
Allergy Awareness and Management Policy Overview This policy is concerned with a whole school approach to the health care management of those members of our school community suffering from specific allergies.
Cow s Milk Free Diet Information For Babies and Children
 Cow s milk allergy occurs when the body s immune (defence) system mistakenly recognises the proteins found in cow s milk as harmful and goes into defence mode by producing an allergic response which is
Cow s milk allergy occurs when the body s immune (defence) system mistakenly recognises the proteins found in cow s milk as harmful and goes into defence mode by producing an allergic response which is
Feeding our children. Anna J Richards NZRD Kidzhealth
 Feeding our children Anna J Richards NZRD Kidzhealth Feeding our children Raising competent eaters and falling off the feeding continuum Competetant eaters have: Positive attitudes about eating and about
Feeding our children Anna J Richards NZRD Kidzhealth Feeding our children Raising competent eaters and falling off the feeding continuum Competetant eaters have: Positive attitudes about eating and about
Medical Conditions Policy
 Medical Conditions Policy Background: Anaphylaxis is a severe, life-threatening allergic reaction. Up to two per cent of the general population and up to 5 percent of young children (0-5yrs) are at risk.
Medical Conditions Policy Background: Anaphylaxis is a severe, life-threatening allergic reaction. Up to two per cent of the general population and up to 5 percent of young children (0-5yrs) are at risk.
ImuPro shows you the way to the right food for you. And your path for better health.
 Your personal ImuPro Screen + documents Sample ID: 33333 Dear, With this letter, you will receive the ImuPro result for your personal IgG food allergy test. This laboratory report contains your results
Your personal ImuPro Screen + documents Sample ID: 33333 Dear, With this letter, you will receive the ImuPro result for your personal IgG food allergy test. This laboratory report contains your results
Food Allergy Risk Minimisation Policy
 Food Allergy Risk Minimisation Policy April 07 Food Allergy Risk Minimisation Policy BACKGROUND Food allergy occurs in around 1 in 20 children. Fortunately, the majority of food allergies are not severe
Food Allergy Risk Minimisation Policy April 07 Food Allergy Risk Minimisation Policy BACKGROUND Food allergy occurs in around 1 in 20 children. Fortunately, the majority of food allergies are not severe
ALLERGY AND ANAPHYLAXIS POLICY
 ALLERGY AND ANAPHYLAXIS POLICY PURPOSE The purpose of this Policy is to provide a safe environment for students with allergies and anaphylaxis as far as reasonably practicable. This Policy is focused on
ALLERGY AND ANAPHYLAXIS POLICY PURPOSE The purpose of this Policy is to provide a safe environment for students with allergies and anaphylaxis as far as reasonably practicable. This Policy is focused on
EC Questionnaire on young- child formulae (Ref: Ares (2014) )
 )") EC Questionnaire on young- child formulae (Ref: Ares (2014)1732912) Response from: Helen Crawley, First Steps Nutrition Trust (www.firststepsnutrition.org) A. Market data In the UK young child formulae
EC Questionnaire on young- child formulae (Ref: Ares (2014)1732912) Response from: Helen Crawley, First Steps Nutrition Trust (www.firststepsnutrition.org) A. Market data In the UK young child formulae
PUREED MEAL IDEAS FOLLOWING BARIATRIC SURGERY
 PUREED MEAL IDEAS FOLLOWING BARIATRIC SURGERY PATIENT INFORMATION LEAFLET Department of Nutrition and Dietetics Sunderland Royal Hospital 1 Why the puree diet is so important You must follow a strict puree
PUREED MEAL IDEAS FOLLOWING BARIATRIC SURGERY PATIENT INFORMATION LEAFLET Department of Nutrition and Dietetics Sunderland Royal Hospital 1 Why the puree diet is so important You must follow a strict puree
Primary Care Update January 26 & 27, 2017 Celiac Disease: Concepts & Conundrums
 Primary Care Update January 26 & 27, 2017 Celiac Disease: Concepts & Conundrums Alia Hasham, MD Assistant Professor Division of Gastroenterology, Hepatology & Nutrition What is the Preferred Initial Test
Primary Care Update January 26 & 27, 2017 Celiac Disease: Concepts & Conundrums Alia Hasham, MD Assistant Professor Division of Gastroenterology, Hepatology & Nutrition What is the Preferred Initial Test
The speaker had sole editorial control over the content in this slide deck.
 Nutricia Paediatric Food Allergy Expert Meeting The speaker had sole editorial control over the content in this slide deck. Any views, opinions or recommendations expressed in the slides are solely those
Nutricia Paediatric Food Allergy Expert Meeting The speaker had sole editorial control over the content in this slide deck. Any views, opinions or recommendations expressed in the slides are solely those
Cow s Milk Allergy: The Facts
 Cow s Milk Allergy: The Facts What is cow s milk allergy? What are the symptoms? What you should bear in mind when managing cow s milk allergy. This factsheet aims to answer some of the questions which
Cow s Milk Allergy: The Facts What is cow s milk allergy? What are the symptoms? What you should bear in mind when managing cow s milk allergy. This factsheet aims to answer some of the questions which
This Product May Contain Trace Amounts of Peanuts Educating Families & Patients About Food Allergies
 This Product May Contain Trace Amounts of Peanuts Educating Families & Patients About Food Allergies Kenya Beard EdD GNP-C NP-C ACNP-BC K Beard & Associates, LLC Assistant Professor Hunter College kenya@kbeardandassociates.com
This Product May Contain Trace Amounts of Peanuts Educating Families & Patients About Food Allergies Kenya Beard EdD GNP-C NP-C ACNP-BC K Beard & Associates, LLC Assistant Professor Hunter College kenya@kbeardandassociates.com
Food allergy in children. Jan Sinclair Paediatric Allergy and Clinical Immunology Starship Children s Hospital
 Food allergy in children Jan Sinclair Paediatric Allergy and Clinical Immunology Starship Children s Hospital Aims Understand something of the epidemiology of childhood food allergy in NZ Review an approach
Food allergy in children Jan Sinclair Paediatric Allergy and Clinical Immunology Starship Children s Hospital Aims Understand something of the epidemiology of childhood food allergy in NZ Review an approach
From diagnosis to weaning and beyond
 A parent s guide to cow s milk allergy: From diagnosis to weaning and beyond By: Rosan Meyer (PhD) and Tanya Wright (BSc Hons, MSc Allergy), specialist paediatric allergy dietitians; Carina Venter (PhD),
A parent s guide to cow s milk allergy: From diagnosis to weaning and beyond By: Rosan Meyer (PhD) and Tanya Wright (BSc Hons, MSc Allergy), specialist paediatric allergy dietitians; Carina Venter (PhD),
Cow s milk protein allergy in children
 Cow s milk protein allergy in children Nicholas Ware UCL Institute of Child Health CPD verifiable Abstract CMPA (Cow s Milk Protein Allergy) is a relatively common condition in infancy that often presents
Cow s milk protein allergy in children Nicholas Ware UCL Institute of Child Health CPD verifiable Abstract CMPA (Cow s Milk Protein Allergy) is a relatively common condition in infancy that often presents
rgies_immune/food_allergies.html
 http://www.kidshealth.org/teen/diseases_conditions/alle rgies_immune/food_allergies.html Food Allergies Peter had always loved seafood, so he was surprised one day when he noticed his mouth tingling after
http://www.kidshealth.org/teen/diseases_conditions/alle rgies_immune/food_allergies.html Food Allergies Peter had always loved seafood, so he was surprised one day when he noticed his mouth tingling after
Living with Coeliac Disease Information & Support is key
 Living with Coeliac Disease Information & Support is key Mary Twohig Chairperson Coeliac Society of Ireland What is Coeliac Disease? LIVING WITH COELIAC DISEASE Fact Not Fad Auto immune disease - the body
Living with Coeliac Disease Information & Support is key Mary Twohig Chairperson Coeliac Society of Ireland What is Coeliac Disease? LIVING WITH COELIAC DISEASE Fact Not Fad Auto immune disease - the body
Gluten Sensitivity Fact from Myth. Disclosures OBJECTIVES 18/09/2013. Justine Turner MD PhD University of Alberta. None Relevant
 Gluten Sensitivity Fact from Myth Justine Turner MD PhD University of Alberta Disclosures None Relevant OBJECTIVES Understand the spectrum of gluten disorders Develop a diagnostic algorithm for gluten
Gluten Sensitivity Fact from Myth Justine Turner MD PhD University of Alberta Disclosures None Relevant OBJECTIVES Understand the spectrum of gluten disorders Develop a diagnostic algorithm for gluten
a) all students and staff with a life threatening allergy (anaphylaxis) are entitled to safe and healthy learning and working environments.
 all students and staff with a life threatening allergy (anaphylaxis) are entitled to safe and healthy learning and working environments.") Title: ANAPHYLACTIC REACTIONS Adopted: December 1, 2015 Reviewed: February 2018 Revised: Authorization: Sabrina s Law POLICY It is the policy of the Bloorview School Authority that: a) all students and
Title: ANAPHYLACTIC REACTIONS Adopted: December 1, 2015 Reviewed: February 2018 Revised: Authorization: Sabrina s Law POLICY It is the policy of the Bloorview School Authority that: a) all students and
Milk. Allergy. Intolerance. in Infants. Advisory panel
 Milk Book Text 2/24/05 1:18 PM Page 1 & Milk Allergy Intolerance in Infants and Children Advisory panel Chairperson Professor Terry D Bolin MD(NSW), BS(Syd), FRACP, FRCP(Lond), FRCP(Edin), DCH(Lond), President,
Milk Book Text 2/24/05 1:18 PM Page 1 & Milk Allergy Intolerance in Infants and Children Advisory panel Chairperson Professor Terry D Bolin MD(NSW), BS(Syd), FRACP, FRCP(Lond), FRCP(Edin), DCH(Lond), President,
WHY IS THERE CONTROVERSY ABOUT FOOD ALLERGY AND ECZEMA. Food Allergies and Eczema: Facts and Fallacies
 Food Allergies and Eczema: Facts and Fallacies Lawrence F. Eichenfield,, M.D. Professor of Clinical Pediatrics and Medicine (Dermatology) University of California, San Diego Rady Children s s Hospital,
Food Allergies and Eczema: Facts and Fallacies Lawrence F. Eichenfield,, M.D. Professor of Clinical Pediatrics and Medicine (Dermatology) University of California, San Diego Rady Children s s Hospital,